

Dal 2010 ad oggi si sono laureati 870 giovani medici ugandesi, che oggi operano in tutti i 40 distretti dell’Uganda. La Facoltà di Gulu, sorella della Federico II, ha dato e continua a dare un contributo sostanziale alla cura del popolo ugandese, con particolare attenzione a Madri e Bambini.
GULU-NAP 20 anni dopo! il vostro contributo non è andato a vuoto
GULUNAP: 20 anni dopo!
Il 4 novembre 2004 abbiamo inaugurato la
Facoltà di Medicina alla Università di Gulu nel Nord Uganda. Nella regione,
devastata da una guerra orribile, risiedevano circa 6 milioni di Ugandesi
serviti scarsamente da circa 20 medici.
Dal 2004 al 2010 30 Docenti della Facoltà di
Medicina Federico II hanno eseguito volontariamente stage formativi alla
neonata Facoltà di Gulu, facendo corsi compatti. Sono stati formati 12 docenti
Ugandesi in varie discipline ed è stata costruita la struttura con un fondo di
contropartita della Cooperazione Italiana. La città di Napoli ha raddoppiato
questo fondo con contributi spontanei.
Dal 2010 ad oggi si sono laureati 870 giovani
medici ugandesi, che oggi operano in tutti i 40 distretti dell’Uganda. La
Facoltà di Gulu, sorella della Federico II, ha dato e continua a dare un
contributo sostanziale alla cura del popolo ugandese, con particolare
attenzione a Madri e Bambini.
LA STORIA DI ALCUNI LAUREATI DEL 2010-11
‘PIONIERI’ DI GULU-NAP
1. Il Dr. Venice Omona è primario della Pediatria
del ‘St. Mary’s Hospital Lacor’ con 200 posti letto ed un reparto tumori
infantili. Dal novembre 2023 ha aperto un nuovo Reparto di Neonatologia e
Terapia Intensiva Neonatale ed è attualmente, per 4 mesi, ospite della Federico
II presso la TIN del Prof. Francesco Raimondi per perfezionarsi in questo
settore.
2. Il Dr. Sylvester Ndsambiya è il primo Chirurgo Ortopedico del Nord Uganda e fa circa 1850 interventi importanti all’anno al St.
Mary’s Hospita di Lacor (si è formato anche a Bolzano per 4 mesi).
3. Il Dr. Godfrey Smart è Chirurgo e Direttore Generale dell’Ambrosoli Hospital di Kalongo, che serve una vasta regione povera
periferica ed ha inaugurato, con la Fondazione Ambrosoli, una Nuova Pediatra con 80 posti letto ed una neonatologia
4. Il Dr. Okello Bosko Otuu, specialista in Ginecologia-Ostetricia, ha aperto nella città di Kitgum un Maternity and Health Center, dove
partoriscono diverse centinaia di donne. Dal 2020, con il sostegno della
Associazione INFANZIA ONLUS Napoli, ha costruito un edificio con 9 aule per una
Scuola di Ostetriche con 60 allieve/anno, in un’area ove la Mortalità Materna è
circa 100 volte maggiore che in Italia.
5. I due ospedali del Nord Uganda (St. Mary’s Lacor ed Ambrosoli Kalongo) hanno partecipato per 3 anni ad un progetto, incoraggiato dalla
Cooperazione Italiana, di Results Based Financing, mediante il quale il
personale ospedaliero riceve ogni 3 mesi un bonus economico significativo in
base ad i punteggi di qualità raggiunti ogni 3 mesi, valutati da una
commissione esterna. Il Prof. Luigi Greco ha sviluppato gli obiettivi da
raggiungere insieme al personale. Nel triennio 2018-2020 il livello di qualità
dei servizi resi ai pazienti è aumentato dall’iniziale 40-50% del target all’
87-92% del target in aree di struttura, gestione, capacità diagnostiche e
terapeutiche. Dopo 4 anni dalla fine del progetto iniziale, abbiamo verificato,
nel febbraio del 2024, che il livello di performance si è mantenuto elevato
(88-95%) in tutte le aree valutate. Gli studenti ugandesi GULU-NAP e gli
specializzandi italiani hanno avuto ed hanno ancora un ruolo importante nella
promozione di obiettivi di qualità del servizio reso. Qualità di servizio che
in un reparto dove muoiono 2-3 bambini al giorno, significa, non raramente, la differenza tra la vita e la morte.
6.
Cinque semplici azioni per
ridurre la Mortalità Materna: in Uganda
il tasso di mortalità legata al parto è circa 100 maggiore di quello del nostro
mondo (350/100.000), peggiorato con la chiusura dei trasporti dovuta alla
pandemia:
1. 4 pause per un Parto Sicuro OMS (3)
2.
Ridurre l’insufficienza di vitamina D 25 nelle donne in gravidanza (4)
3.
Prevenire la sepsi puerperale con un’iniezione di azitromicina (5,6), adottare
acido tranexamico per ridurre l’emorragia. (7)
4.
Facilitare l’invio e la gestione precoce stimando al primo contatto con la
madre il rischio di un esito sfavorevole (8)
5.
Facilitare il parto vaginale considerando il dispositivo di erogazione ODON
(9,10,11). Applicare Ellavi Baloon per gestire l’emorragia post parto (12).
GULU-NAP 20 ANNI DOPO !!! Il vostro
contributo non è andato a vuoto.
“Result Based
Financing, a change engine for paediatric services”
Reengineering
pediatric services with Results-Based Financing (RBF) involves restructuring
healthcare delivery systems to improve efficiency, quality, and patient
outcomes, particularly in under-resourced areas like Northern Uganda. RBF
programs typically provide financial incentives to healthcare providers based
on the achievement of predefined results or outcomes, such as improved health
metrics among the pediatric population.
This study considers
a theoretical setting of healthcare RBF and then applies its main findings to
two empirical cases, concerning S. Mary’s Lacor Hospital in Gulu and Dr.
Ambrosoli’s Memorial Hospital in Kalongo before and after the Covid-19 pandemics (from 2018 to 2024).
The success of RBF programs depends on
several factors, including the design of the incentive schemes, the context in
which they are implemented, and the capacity of health facilities to respond to
the incentives. Moreover, careful consideration must be given to ensure that
RBF programs do not inadvertently create perverse incentives or widen health
disparities.
Within
this framework, the paper’s research question is to examine the Long-Term
Effects of RBF Intervention in Children’s Wards in two main Northern Uganda
hospitals (Lacor and Kalongo) in a pre- and post- Covid timeframe, from 2018 to
2024.
The
study follows an IMRAD pattern and is structured as follows: after a short
literature analysis, we present a model backed by empirical findings that
precede a discussion and conclusion.
4.1.1.
Lacor Hospital
Fig. 1
shows the percentage of the target score for the domain of Structure of the
ward and Management of the Ward plus the action to preserve Hygiene and prevent
infections at Lacor.
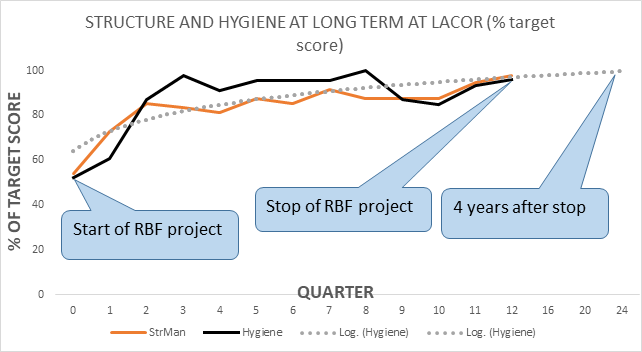
At Lacor
the first year of the project was dedicated to covering the gaps in the
respective domains, reaching, at the end of the first year (quarter 4) scores
quite close to the set target. After the stop of the project (2020) there was
no decay of the performance: at the point assessment of 2024, four years after
the stop, the scores were very close to the target (see Table 1).
Fig. 2
shows the performance (as % of target score) in the domain of Clinical
Management of patients, Emergency readiness, and training of students (nurses,
medical doctors, and post-graduates) at Lacor.
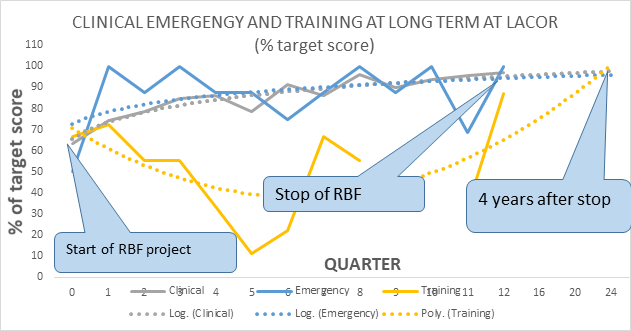
The pattern is like the one observed in Fig. 1: during the first year a significant
performance improvement, which remained stable up to the end of the project
(2020) and is still kept four years after the end. A special note should be
dedicated to the domain of training: during the second and third years, the
occasional absence of senior supervisors and the uncontrolled rotation of
students (especially medical) made this activity unstable. By 2024 also
training appeared to be stabilized at a high level of performance.
4.1.2.Kalongo Hospital
Fig. 3
shows the percentage of the target score for the domain of Structure of the
ward and Management of the Ward plus the action to preserve Hygiene and prevent
infections at Kalongo.
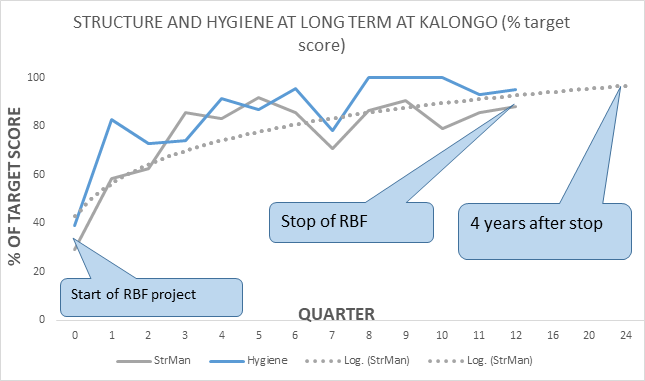
At Kalongo
the first year of the project was dedicated to covering the gaps in the
respective domains, investing the resources gained by the RBF project, in the
amendment and maintenance of the basic structure of the children’s ward. In the
second year (quarters 5-8) the improvement toward the target became sensible,
to reach in the third-year scores very close to the final objectives. After the
stop of the project (2020) there was no decay of the performance: at the point
assessment of 2024, four years after the stop, the scores were very close to
the target (see Table 1).
Fig. 4
shows the performance (as % of target score) in the domain of Clinical
Management of patients, Emergency readiness, and training of students (nurses,
medical doctors, and post-graduates) at Kalongo.
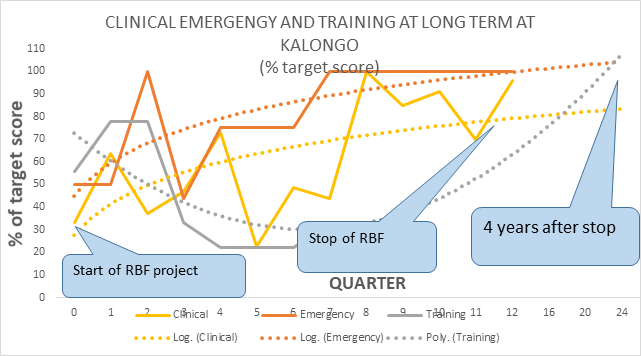
The
inconstant presence of the pediatrician affected considerably the stability of
the performance of clinical management and the training of students. Especially
in the second-year supervision and guidance appeared to be unstable,
significantly affecting performance. By the third year, a significant
improvement was observed, which was maintained as far as four years after the
stop of the project.
Fig. 5
shows the improvement of quality scores as a percentage of the starting scores
(at time 0 start of the project) either of the scores reached at the end of the
project (2020) as well of the scores four years after the end of the project
(2024) for Lacor and Kalongo Children’s Wards. (‘20’ = Scores 2020-scores of
2018)*100/Scores of 2018) , (‘24’ = Scores 2024-scores of 2018)*100/Scores of
2018).
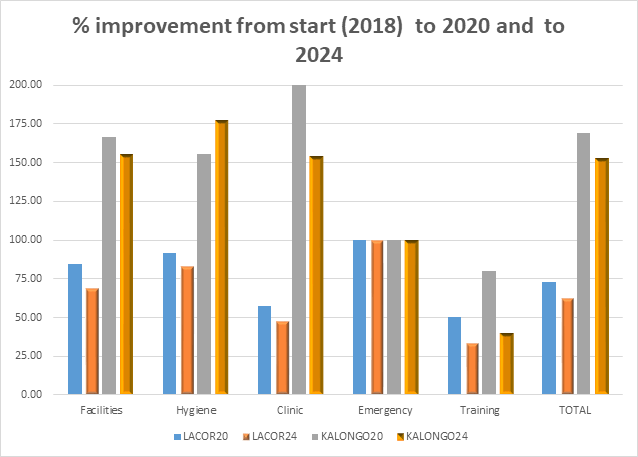
The
% improvement in performance in all domains was greater in Kalongo than in
Lacor since the starting point of this hospital was significantly lower
compared to Lacor. However, it is intriguing to observe the relative stability
of the improvement after four years by the end of the project. For example, in
Kalong there was a + 150% of the scores from the start of 2018 to the end
(2020) for structure management and hygiene, but still a stable 150%
improvement from 2018 to 2024 after the stop of the project. The domain of
emergency was stabilized early and kept on a long time, while the area of
training could improve less in Kalongo than at Lacor, due to the inconstant
presence of supervision.