

On 4 November 2004, we inaugurated the Faculty of Medicine at the University of Gulu in Northern Uganda. In the region, ravaged by a horrific war, some 6 million Ugandans resided, poorly served by around 20 doctors.
From 2004 to 2010, 30 lecturers from the Federico II Faculty of Medicine voluntarily carried out training placements at the newly established Faculty of Medicine in Gulu, doing compact courses. Twelve Ugandan lecturers were trained in various disciplines and the structure was built with a counterpart fund from the Italian Cooperation. The city of Naples doubled this fund with spontaneous contributions.
Since 2010, 870 young Ugandan doctors have graduated and are now working in all 40 districts of Uganda. The Faculty of Gulu, sister of the Federico II, has made and continues to make a substantial contribution to the care of the Ugandan people, with particular attention to Mothers and Children.
THE STORY OF SOME 2010-11 GRADUATES ‘PIONEERS’ OF GULU-NAP
- Dr. Venice Omona is head of paediatrics at ‘St. Mary’s Hospital Lacor’ with 200 beds and a children’s cancer ward. Since November 2023, he has opened a new Neonatology and Neonatal Intensive Care Unit and is currently, for 4 months, a guest of the Federico II at the NICU of Prof. Francesco Raimondi to perfect his skills in this area.
- Dr. Sylvester Ndsambiya is the leading Orthopaedic Surgeon in Northern Uganda and performs about 1850 major operations a year at St. Mary’s Hospita in Lacor (he also trained in Bolzano for 4 months).
- Dr. Godfrey Smart is Surgeon and General Director of the Ambrosoli Hospital in Kalongo, which serves a vast peripheral poor region and has inaugurated, with the Ambrosoli Foundation, a New Paediatric Hospital with 80 beds and a neonatology unit
- Dr. Okello Bosko Otuu, a specialist in Gynaecology-Obstetrics, has opened a Maternity and Health Centre in the city of Kitgum, where several hundred women give birth. Since 2020, with the support of the Naples INFANZIA ONLUS Association, he has built a building with 9 classrooms for a Midwives School with 60 pupils/year, in an area where Maternal Mortality is about 100 times higher than in Italy.
- The two hospitals in Northern Uganda (St. Mary’s Lacor and Ambrosoli Kalongo) have participated for 3 years in a project, encouraged by the Italian Cooperation, of Results Based Financing, through which the hospital staff receive a significant economic bonus every 3 months based on the quality scores achieved every 3 months, assessed by an external commission. Prof. Luigi Greco developed the objectives to be achieved together with the staff. In the three-year period 2018-2020, the quality level of services rendered to patients increased from the initial 40-50% of the target to 87-92% of the target in the areas of structure, management, diagnostic and therapeutic capabilities. Four years after the end of the initial project, we verified in February 2024 that the performance level remained high (88-95%) in all areas assessed. Ugandan GULU-NAP students and Italian trainees had and still have an important role in promoting quality of service objectives. Quality of service that in a ward where 2-3 children die every day, means, not infrequently, the difference between life and death.
- Five Simple Actions to Reduce Maternal Mortality: In Uganda, the maternal mortality rate is about 100 higher than in our world (350/100,000), worsened with the closure of transport due to the pandemic:
- 4 breaks for Safe Childbirth WHO (3)
- Reducing Vitamin D 25 insufficiency in pregnant women (4)
- Prevent puerperal sepsis with an injection of azithromycin (5,6), adopt tranexamic acid to reduce bleeding. (7)
- Facilitate early referral and management by estimating at first contact with the mother the risk of an unfavourable outcome (8)
- Facilitate vaginal delivery by considering the ODON delivery device (9,10,11). Apply Ellavi Baloon to manage postpartum haemorrhage (12).
GULU-NAP 20 YEARS LATER !!! Your contribution has not gone in vain.
“Result Based. Financing, a change engine for paediatric services”
Reengineering pediatric services with Results-Based Financing (RBF) involves restructuring healthcare delivery systems to improve efficiency, quality, and patient outcomes, particularly in under-resourced areas like Northern Uganda. RBF programs typically provide financial incentives to healthcare providers based on the achievement of predefined results or outcomes, such as improved health metrics among the pediatric population.
This study considers a theoretical setting of healthcare RBF and then applies its main findings to two empirical cases, concerning S. Mary’s Lacor Hospital in Gulu and Dr. Ambrosoli’s Memorial Hospital in Kalongo before and after the Covid-19 pandemics (from 2018 to 2024).
The success of RBF programs depends on several factors, including the design of the incentive schemes, the context in which they are implemented, and the capacity of health facilities to respond to the incentives. Moreover, careful consideration must be given to ensure that RBF programs do not inadvertently create perverse incentives or widen health disparities.
Within this framework, the paper’s research question is to examine the Long-Term Effects of RBF Intervention in Children’s Wards in two main Northern Uganda hospitals (Lacor and Kalongo) in a pre- and post- Covid timeframe, from 2018 to 2024.
The study follows an IMRAD pattern and is structured as follows: after a short literature analysis, we present a model backed by empirical findings that precede a discussion and conclusion.
4.1.1. Lacor Hospital
Fig. 1 shows the percentage of the target score for the domain of Structure of the ward and Management of the Ward plus the action to preserve Hygiene and prevent infections at Lacor.
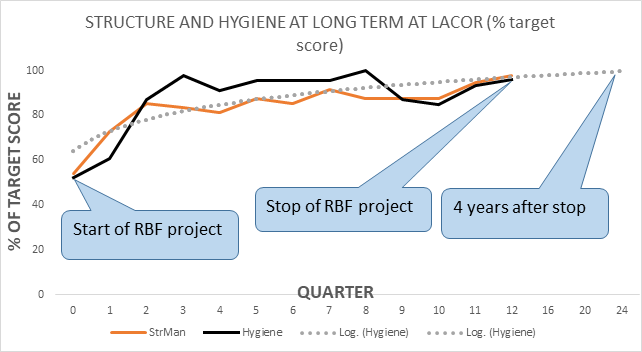
At Lacor the first year of the project was dedicated to covering the gaps in the respective domains, reaching, at the end of the first year (quarter 4) scores quite close to the set target. After the stop of the project (2020) there was no decay of the performance: at the point assessment of 2024, four years after the stop, the scores were very close to the target (see Table 1).
Fig. 2 shows the performance (as % of target score) in the domain of Clinical Management of patients, Emergency readiness, and training of students (nurses, medical doctors, and post-graduates) at Lacor.
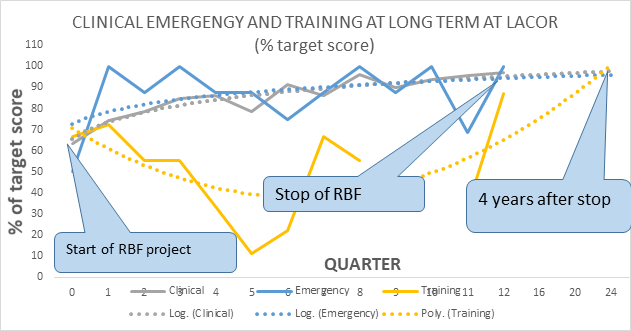
The pattern is like the one observed in Fig. 1: during the first year a significant performance improvement, which remained stable up to the end of the project (2020) and is still kept four years after the end. A special note should be dedicated to the domain of training: during the second and third years, the occasional absence of senior supervisors and the uncontrolled rotation of students (especially medical) made this activity unstable. By 2024 also training appeared to be stabilized at a high level of performance.
4.1.2.Kalongo Hospital
Fig. 3 shows the percentage of the target score for the domain of Structure of the ward and Management of the Ward plus the action to preserve Hygiene and prevent infections at Kalongo.
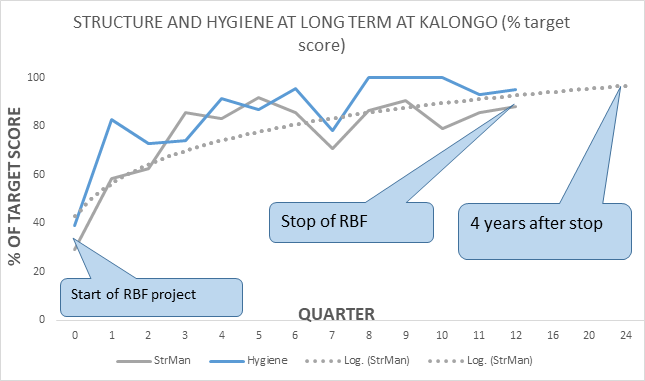
At Kalongo the first year of the project was dedicated to covering the gaps in the respective domains, investing the resources gained by the RBF project, in the amendment and maintenance of the basic structure of the children’s ward. In the second year (quarters 5-8) the improvement toward the target became sensible, to reach in the third-year scores very close to the final objectives. After the stop of the project (2020) there was no decay of the performance: at the point assessment of 2024, four years after the stop, the scores were very close to the target (see Table 1).
Fig. 4 shows the performance (as % of target score) in the domain of Clinical Management of patients, Emergency readiness, and training of students (nurses, medical doctors, and post-graduates) at Kalongo.
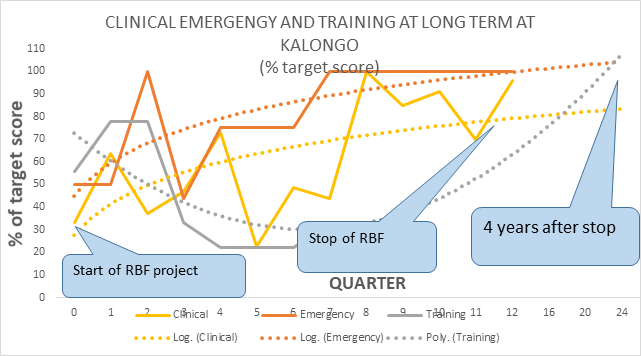
The inconstant presence of the pediatrician affected considerably the stability of the performance of clinical management and the training of students. Especially in the second-year supervision and guidance appeared to be unstable, significantly affecting performance. By the third year, a significant improvement was observed, which was maintained as far as four years after the stop of the project.
Fig. 5 shows the improvement of quality scores as a percentage of the starting scores (at time 0 start of the project) either of the scores reached at the end of the project (2020) as well of the scores four years after the end of the project (2024) for Lacor and Kalongo Children’s Wards. (’20’ = Scores 2020-scores of 2018)*100/Scores of 2018) , (’24’ = Scores 2024-scores of 2018)*100/Scores of 2018).
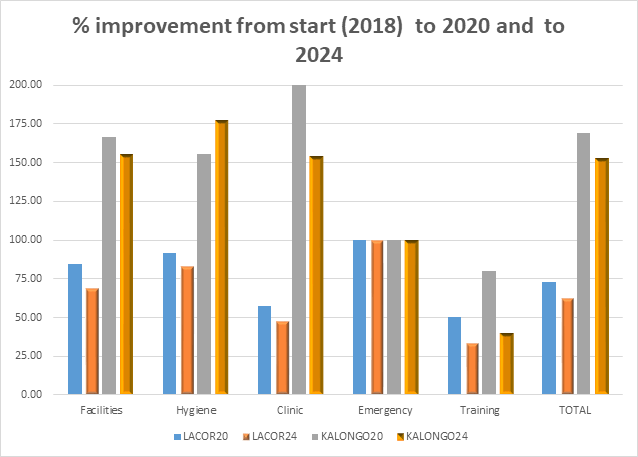
The % improvement in performance in all domains was greater in Kalongo than in Lacor since the starting point of this hospital was significantly lower compared to Lacor. However, it is intriguing to observe the relative stability of the improvement after four years by the end of the project. For example, in Kalong there was a + 150% of the scores from the start of 2018 to the end (2020) for structure management and hygiene, but still a stable 150% improvement from 2018 to 2024 after the stop of the project. The domain of emergency was stabilized early and kept on a long time, while the area of training could improve less in Kalongo than at Lacor, due to the inconstant presence of supervision.
Download Result Based. Financing, a change engine for paediatric services in pdf file
Photo gallery